
Introduction
For the past several decades the suggested protection for any real or potential loss of mandibular and/or maxillary arch length has been the placement of a fixed lingual arch (LA) or a fixed/removable lingual arch (FRLA). Other appliances have also been in vogue…among them the Ricketts Utility Arch or “U” arch.
This blog attempts to enable the practitioner to make wise choices when arch length management is under consideration. The soldered lingual arch is likely the first appliance to be considered, followed by the fixed/removable lingual arch (FRLA). While the Ricketts Utility Arch has numerous functions, this appliance appears to be utilized primarily by the orthodontic practitioner. However, there has been a steady movement toward the use of a “U” arch by non-extraction practitioners as a 1st Phase appliance. The use of a “U” arch by Pediatric Dental practitioners for arch length control makes sense because loss of arch length is common and the regaining of space for erupting premolars and canines is of utmost importance. The lingual arch holds arch length quite well, however this appliance cannot easily regain lost arch length in the mixed dentition phase of oro-dental maturation. The FRLA has some benefits over the soldered lingual arch and its use in the hands of well-informed practitioners can result in arch length improvement. In general, the discrete bends required to increase arch length will require substantial skill in archwire bending and manipulation. Auxiliaries soldered to lingual archwires can also be helpful and in some cases the lost arch length can be recovered. There are alternatives to the lingual arch that can substantially improve upon mixed dentition arch length management.
The Ricketts Utility Arch

The primary molars retain a remarkable capacity to hold arch length. However, any mesial movement of the first permanent molar will encroach upon arch length and can substantially decrease the space required for normal eruption of the premolars. If bilateral mesial movement is observed, the complication is multiplied…often to a severe degree. The distal surface of the second primary molar is the eruption “guide” for the 1st permanent molar and serves many important functions in the mixed dentition until it exfoliates at approximately 12 years of age. In addition, any lingual movement of the mandibular incisors will also impinge upon the arch lengthMany modifications of the original “U” arch design have been utilized to protect or modify the arch length in the mixed dentition. The design of the “U” arch appliance is not complicated and its use in the mixed dentition for arch length management by Pediatric Dentists should not be overlooked.The properly designed passive or activated “U” arch has the following advantages.
Advantages of the Utility Arch
1. Uprighting and rotational control of the permanent molar.
2. Control of the lower incisor segment…including intrusion, labial or lingual movement, and rotational control.
3. Ease of adjustment. Easily accessed anterior bracket engagement and no “tie back” on the permanent molar.
4. Sectional management of the anterior and/or posterior segments that bypass the erupting premolars and canines.
5. An easily formed arch wire that utilizes a buccal entry of attachment.
6. Each section of the “U” arch…right or left can be adjusted independently.

The Intact Primary Dentition
A Diagnostic Protocol prior to Treatment
A basic set of pretreatment records is essential. Many of these requirements can be requested by prescription to laboratories that specialize in pre-treatment records.
1. Full Mouth Periapical X-Rays with Bitewing films
2. Lateral Cephalometric X-rays & Panoramic X-Ray
3. Orthodontic trimmed models
4. Intra-oral and extra-oral photographs (lateral and full face)
5. A lateral Cephalometric Tracing – Ricketts tracing recommended
The Transitional Dentition
When the primary teeth loosen and the new permanent incisor erupts, the dentition is in transition. The transition to all permanent teeth will be complete at about the 12th year excluding the third molars. During the transitional phase of oral maturation the position of the first permanent molar must be protected. Any oral pathology that allows a mesial shift of the first permanent molar or lingual displacement of the mandibular incisor segment must be avoided.
Loss of Arch Length - Etiology
1. Interproximal caries with mesial shift of posterior quadrants.
2. Early loss of primary canines with midline shift.
3. Extraction of primary teeth.
4. Ankylosis of primary molars.
5. Ectopic eruption of maxillary 1st permanent molars.

Mesial Shift due to proximal caries
Early treatment for loss of arch length is essential if the patient is to avoid extended orthodontic treatment that often requires the extraction of premolars. Severe loss of arch length in the mixed dentition is often unable to be treated non-extraction and requires a serial extraction protocol. The potential loss of four premolars can solve a large arch length discrepancy, however an extraction protocol will require orthodontic management over the course of many months.

Point "A" depicted by red arrow

Point "Pog" depicted by red arrow
Ricketts Cephalometric Landmarks
Note that a line drawn from Point A to Pog should lie I millimeter behind the incisal tip of the lower incisor...on average. The potential answer to this conundrum is the use at the appropriate time of a Ricketts designed Utility Arch.The “U” arch may be activated to produce labial movement of the mandibular incisors if they are lingually inclined. In addition, the permanent molar can often be bucally rotated to gain some small amount of arch length increase.Using cephalometric standards for the mandibular incisor position to the APo line, a proposed labial advancement can be achieved. The Caucasian APo line standard is a +1 millimeter S.D. 2. Other standards can also be applied at the discretion of the professional.
Hispanic Standard APo +4.7 mm - Standard Deviation
Japanese Standard APo +3 mm - Standard Deviation 2
African American Standard APo +5.2 mm - Standard Deviation 2
Rationale
If the lower incisors can be moved forward the resulting increase in arch length will be 2-millimeter gain for each 1 millimeter of forward movement of the mandibular incisor. The 2 to 1 “rule of thumb” is straightforward and comes from the dicta of the Steiner Cephalometric Analysis. Forward movement of the incisor segment is often able to convert an extraction case into a non-extraction diagnosis. But in addition, the uprighting or distal rotation of the mandibular molars can also create small amount of additional arch length.
Early treatment for loss of arch length is essential if the patient is to avoid extended orthodontic treatment that often requires the extraction of premolars. Severe loss of arch length in the mixed dentition is often unable to be treated non-extraction and requires a serial extraction protocol.
Leeway Space

The Early Mixed Dentition
It is well known that the mesio-distal dimension of the second primary molar is larger than the succedaneous bicuspid. There is a tendency to allow mesial movement of the first permanent molar because some practitioners believe that it is appropriate to allow the mesial movement of the molar to improve upon the Class I molar relationship.
It is true that on occasion mesial movement in the late mixed dentition occurs, but that fact should not condone mesial movement that impacts the arch length in the early mixed dentition phase of occlusal development. According to many observers the “leeway space” is utilized in its entirety by the distal movement of the erupting canine and premolars. The failure to keep the arch length intact in the early mixed dentition will often result in a crowded arch.
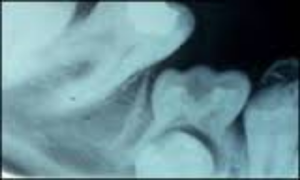
Mesial Shift of First Molar over an Ankylosed Primary Molar
Mesial Shift of Posterior Quadrants
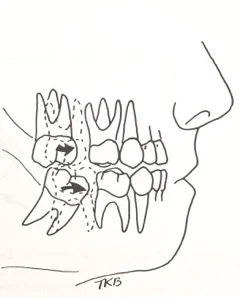
Mesial shift of 1st Permanent Molar - Courtesy Dr. T. K. Barber
The loss of contact between the primary molars due to extensive carious involvement allows mesial movement of the permanent first molar and jeopardizes the arch length that is required for late mixed dentition eruption. The loss of contact is an important factor in the etiology of a crowded arch at maturation. The timing of intervention requires close observation of the developing dentition since substantial loss of arch length cannot be easily recovered. Many practitioners tend to closely guard the mandibular arch length since distalization of the mandibular molars often requires heroic action. Small amounts of arch length loss can often be recovered at the early mixed dentition stage, however larger amounts of loss often create the need for the extraction of a bicuspid in all four quadrants. In an overall sense, the critical nature of adequate arch length in every patient requires that the practitioner must use an appropriate appliance to protect the developing dentition when early loss of primary teeth has occurred.
Premature Loss of the Mandibular Primary Canine
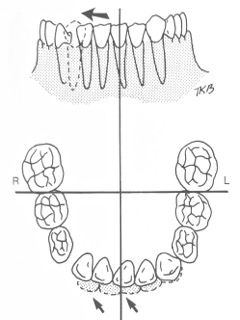
Premature loss of a Primary Canine - Courtesy Dr. T. K. Barber
The eruption of the mandibular incisors is often the first visible evidence that the dentition is in transition. When a primary mandibular canine exfoliates prematurely, the permanent lateral often erupts into a more distal relationship skewing the midline. This modification of the midline is a very early indication that the arch length has been compromised. Often the dental practitioner will recommend that the opposite primary canine be extracted to help maintain the midline relationship. This treatment plan many help to restore the midline alignment but arch length decrease may continue if the mandibular incisors assume a more lingual position. This lingual positioning may be due to abnormal contraction of the Mentalis upon deglutition, or oral habits may also be a contributing factor. Restoring the normal incisor relation to the A to Pog line should be considered as a possible treatment plan for the future. The “U” arch will likely be the first option when a repositioning plan is adopted. If the Mentalis muscle is at fault, bracket placement on the labial surface of the lower incisors will often be a deterrent to aberrant swallowing patterns. Keep in mind that labial repositioning the incisor segments forward one millimeter will result in a two millimeter arch length gain. The two for one relationship cannot be overlooked in managing a maturing mixed dentition.
Labial Movement of the Mandibular Incisors
If the lower incisors erupt into a position that is lingual to their normal position at a +1 to APo, then the arch length is decreased on the 2 to 1 dictum of Dr. Steiner. Lingual eruption is not unusual if the patient has a thumb/finger sucking habit or a modified pattern of deglutition. Tongue thrusting into an anterior open bite tends to allow the incisors to remain depressed and/or lingual to their intended cephalometric location. One the more important “watch-dog” duties of the Pediatric Dentist is to insure that the arch length is not compromised by habits or non-physiologic deglutition. Support for the incisor segment during the early mixed dentition phase is of the utmost importance for correct alignment of the succedaneous dentition.
Loss of Arch Length – Ankylosis
Minimal loss of arch length can easily occur when the posterior primary dentition fails to maintain the correct occlusal height. These molars appear to “submerge” when in actual fact they lack a true periodontal ligament that allows for physiologic eruption at the same rate as their adjoining posterior segments. The “tooth to bone” attachment firmly attaches the primary root to the alveolar bone and often creates arch length inadequacy. The practitioner must however be aware that the early signs of ankylosis should “raise a red flag” that something is amiss. Particularly at fault it the second primary molar that fails to keep pace with the eruption of the 1st permanent molar and the resulting occlusal discrepancy allows a mesial shift when the height of mesial contour over rides the distal contact of the second primary molar. The resulting mesial shift can create a very substantial loss of arch length, particularly when it occurs bilaterally or in several primary molars.
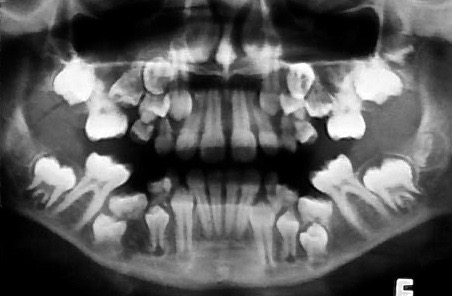
Primary molar ankylosis with complex pathology
The early diagnosis of primary molar ankylosis is an imperative considering that this oral anomaly creates many overriding oral pathologies. Close observation of the offending primary molars can result in an early diagnosis that demands the attention of the practitioner.

Loss of Occlusal Positioning suggesting ankylosis of the first and second primary molar and congenitally missing second bicuspid.
The loss of occlusal height is one of the first hints that this pathology is present. Bitewing x-rays will often be the first subjective sign that this progressive disease is impacting the development of the occlusion. Additional x-rays are indicated to ascertain the presence or absence of the succedaneous dentition. In addition, it may be necessary to prepare a long-term treatment plan that lists the options for early and/or late treatment. It may also be necessary to recommend that lateral cephalograms be taken to use as a reference tool as the oro-facial complex matures. At this time it may also be necessary to determine the facial growth pattern…is it Mesocephalic, Brachycephalic, or Dolichocephalic?
Cephalometrics

Ricketts Lateral Cephalogram
The use of a cephalometric lateral x-ray at the mixed dentition phase of oral development is highly recommended. The early detection of the oro-facial growth facial pattern will give every practitioner the ability to prioritize treatment options and to predict the effect of growth. The Brachycephalic face (low angle) presents with options that may conflict with the treatment options presented by the Dolichocephalic facial (high angle) pattern of growth, while the Mesocephalic face suggests that a more normative treatment plan will be appropriate.
A Cephalometric Mean for the Mandibular Incisor
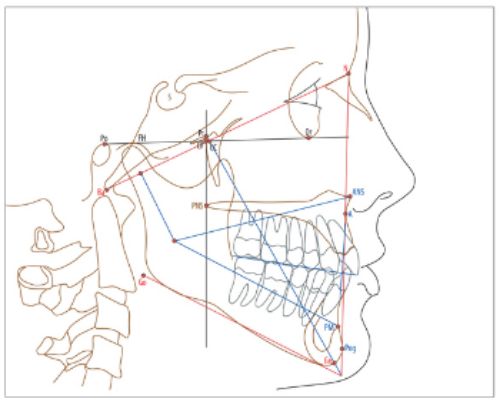
Ricketts Lateral Cephalogram Essential Landmarks

The A to Pog Line
The anterior-posterior position of the mandibular incisors relative to the “A to Pog” or “A” to Po” line is constant throughout life. The Caucasian standard is a plus 1-millimeter with a standard deviation of 2 millimeters. Other ethnic groups have standards that can be used to ascertain the mean and those standards can be used to plan treatment procedures. Many practitioners believe that this measurement is an essential factor in determining the treatment plan prior to instigating appliance therapy in the early mixed dentition. One of the more common results of long-term finger sucking habits is the lingual collapse of the incisor segment. Other landmarks are important in the development of a treatment plan and familiarity with every landmark is essential. The common use of the Bioprogressive Lateral Cephalometric x-ray analysis fits in well with Bioprogressive treatment philosophy. The determination of growth pattern with successive overlays taken every two years will also allow the practitioner to assess treatment success. Essential to the ultimate treatment plan is the determination of the basic growth pattern…whether it is Mesocephalic, Brachycephalic, or Dolichocephalic. Each pattern of growth has its own treatment patterns that point to a successful outcome.
The “U” arch is a utilitarian method that improves on the general usage of the “age-old” lingual arch due to its ability to perform a variety of functions. A more general use of the “”U” arch by practitioners will improve the ability of most practitioners to reposition both posterior and anterior segments of the arch. This appliance will rotate and distalize the first permanent molar, de-rotate and reposition the incisor segments, and allow a segmental approach to early mixed dentition management. The segmental approach allows treatment to be directed to the anterior or posterior segments independently of each other. Varying anchorage positions can facilitate favorable response where required for maximum response.
In the case of primary molar ankylosis, the uprighting of the permanent molar or the maintenance of the arch length with a removable “U” arch could retain the correct arch length during the transitional period of primary to permanent eruption. In addition, it may be prudent to manage the position of the mandibular incisor segment. Subsequently a standard lingual arch may be required to retain the correct arch length.
The Anatomy of a “U” Arch
Anterior Segment – Distal of permanent lateral incisor to the distal of the antimere.
Buccal Bridge – Lateral incisors to the buccal tube of the permanent molar.
Molar Section – The extension into the buccal tube.

The Mandibular “U” arch
Improving Posterior Anchorage
If additional posterior anchorage is desirable, the placement of a lingual arch can support the position of the molar anchorage and deliver anterior force only. If the lingual arch is fixed and removable, the anchorage needs can be added or removed as desired.
It is a basic tenet of Rickett’s philosophy that a segmental approach to treatment allows the erupting permanent bicuspids and canines to be excluded at the early stage of treatment. The subsequent addition of a segmental archwire in the more occlusal slot of the molar tube allows alignment of those teeth independently of the “U” arch. Later finishing of the entire arch can be accomplished with a single archwire either added to the “U” arch or used after the “U” arch is discarded.
Essential to this option is the attachment of brackets with a deeper slot dimension...030…thus enabling the addition of another “piggyback” archwire.

Cross Arch Anchorage plus “U” Arch
Utility Arch Construction
In the past the arch was constructed using a .016 x .016 Elgiloy preformed blank. Some practitioners prefer a stainless archwire that is .016 x .016. A slightly different size is often used in the maxillary arch…the .016 x .022. The permanent molars should be banded, but in some cases a bonded buccal tube may suffice. The mandibular incisors are bonded with twin brackets using a .018 x .025 slot dimension. Some practitioners prefer a greater depth to the slot and recommend a depth of .030. The arch wire engages the mandibular incisors and steps down at the lateral incisor/canine contact approximately 3 to 5 millimeters. It extends distally to the mesial of the molar tube where an occlusal bend of 3 to 4 millimeters for insertion into the molar tube. If the incisors are significantly misaligned, a four-incisor sectional leveling round archwire can be introduced until the entire .016 “U”archwire can be engaged. Some practitioners recommend a 4 to 5 mm step rather than 3 to 4 millimeters.
Ties
Engagement of the archwire into the anterior bracket slots is best accomplished by using elastomeric ties that are easily engaged using a mosquito hemostat. Wire ligatures may be required on occasion.

Activation
The initial insertion of the “U” archwire is ordinarily placed as passive as possible. The incisor segment must be “leveled”, that is the bracket slots must align so that the .016 x .016 archwire can be engaged in the four incisor slots. The distal section that inserts into the buccal tube should also remain passive. The “bridge” section that spans the distance between the molar tube and the contact between primary canine and the permanent lateral incisor must also lie close to the soft tissue. If it is formed too wide it will impinge on the cheek and cause discomfort. The insertion into the buccal tube is not “tied back.” The insertion can be easily pulled out by the patient therefore some warning must be given to the patient. For the first visit it is acceptable to place a slight bend distal to the buccal tube to disallow removal by the patient until after the second visit.
Synopsis
Many practitioners have some difficulty distinguishing tooth movement for specialty practitioners in Pediatric Dentistry versus some Orthodontic practitioners who typically use a “full hookup” in their management of malocclusion. This observer believes that the Pediatric specialist must support an adequate arch length during the mixed dentition period. That fact suggests that some patients who have misalignment due to pathology, mesial movement of permanent molars, or lingual collapse of the permanent incisors must be managed appropriately during the early mixed dentition. When habit patterns are also involved in the misalignment, the management will often fall into the specialty practice of the Pediatric Dentist. The “U” arch is an improvement over lingual arches that can be more difficult to manage particularly when maximum activation is required to control the arch length. If throughout the transition to permanent dentition the arch length is adequate, the permanent teeth will often erupt into a very satisfactory pre-orthodontic alignment.
The emphasis in this commentary is upon the treatment of the mandibular arch since the ultimate orthodontic diagnosis will often hinge upon the lower arch that is more difficult to manage than the components of the maxillary arch. Integral to this concept is the position in space of the mandibular incisors, since the stability and the requirements of arch length are built upon mandibular incisor position with esthetic normalcy. The Steiner 2 for 1 ratio in regard to the incisor position must always be in the mind of a practitioner who observes mandibular collapse associated with habits or poor deglutition physiology.

The “U” Arch – Rickett’s design
The Utility Archwire is an appliance that can hold and to a degree upright the permanent molar and reposition the incisor segment during early mixed dentition should be in the armamentarium of every Pediatric Dentist. It is within our frame of reference to manage and correct early oral pathology that interferes with the normal transitional phase of oro-dental maturation…an objective well worth pursuing for Pediatric Dental patients. If later or second phase treatment is deemed advisable, the early “setup” of the mixed dentition can improve the final outcome of two-phase treatment. The maturation of the Utility Arch into a full Ricketts hookup is a second phase of management that may be required to complete many orthodontic cases. The specialty of Pediatric Dentistry may conclude that early intervention of arch length deficiencies is an important facet of our treatment regimen.
Suppliers
Rocky Mountain Orthodontics www.rmortho.com
Ortho Organizers www.orthoorganizers.com
Ormco www.ormco.com
American Orthodontics www.americanortho.com
Using “You Tube” to Review Construction and use of the “U” arch see:
https://www.youtube.com/watch?v=iW9GomNO0V0
You can search the web for the Ricketts Utility Arch for other related videos. The University of Michigan has several You Tube videos of the appliance and an interview with Dr. Ricketts.